
The process begins with hormone therapy to stimulate the ovaries to produce multiple eggs. This typically involves daily injections of gonadotropins.
During stimulation, about 3 to 5 blood tests and ultrasounds are performed to monitor the growth and development of the follicles (which contain the eggs).
Once the follicles are mature, a trigger shot of hCG or GnRh agonist (intranasal Synarel (r) or subcunateous decapeptyl (r)) is given to prepare for egg retrieval. About 36 hours later, a minor surgical procedure is performed, usually under anesthesia, to collect the eggs through the vaginal wall from the ovaries using a thin needle.
During the egg retrieval, a sperm sample is collected from the male partner or a donor . The sperm is then processed to isolate the healthiest sperm.
The retrieved eggs are combined with the processed sperm in a laboratory dish. Fertilization can occur naturally or through a technique called intracytoplasmic sperm injection (ICSI), where a single sperm is injected directly into an egg.
The fertilized eggs, now called embryos, are cultured for several days (usually 3 to 5 days) to allow them to develop. Embryologists monitor their growth and quality.
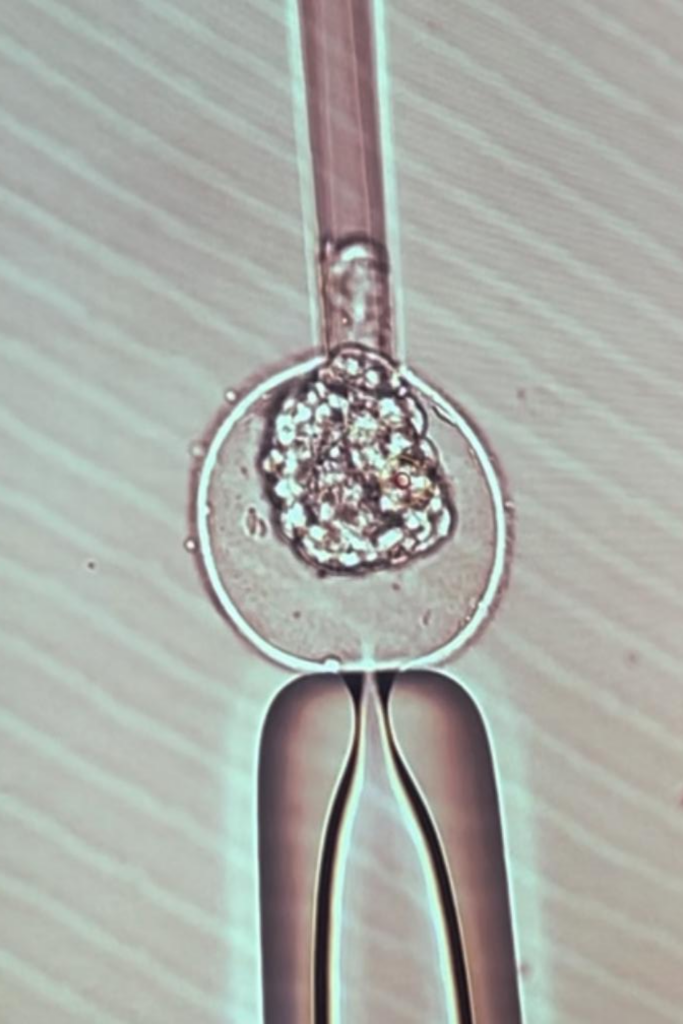
Once the embryos are ready, one is selected for transfer into the woman’s uterus. This is done using a thin catheter and is usually a painless procedure. The other day 5 embryos are frozen
Hormonal support, often in the form of progesterone supplements, is provided to help prepare the uterine lining for implantation.
About 10-14 days after the embryo transfer, a blood test is performed to determine if implantation has occurred and if the woman is pregnant.
If the test is positive, additional monitoring occurs to ensure a healthy pregnancy. If not, the woman may discuss options for future cycles.
The first step involves a thorough evaluation of both partners’ fertility. This may include blood tests, ultrasound examinations, and sperm analysis to determine the underlying causes of infertility and decide if IUI is a suitable treatment option.
To optimize the chances of conception, the woman may be prescribed medications that stimulate her ovaries to produce multiple eggs. Common drugs used for this purpose include clomifene or gonadotropins. The response to these medications is closely monitored with ultrasounds and blood tests to track the growth of follicles (the sacs containing eggs).
Regular ultrasounds are performed to monitor the growth of the follicles. Once the follicles have reached the right size, an injection of human chorionic gonadotropin (hCG) is often given to trigger ovulation, signaling the eggs to be released.
On the day of insemination, a sperm sample is collected from the male partner (or a sperm donor if necessary). The sperm is then processed in the laboratory to separate healthy, motile sperm from the semen. This ensures that the sperm used for insemination are of the highest quality.
Once ovulation is triggered, and the sperm is prepared, the IUI procedure itself takes place. The sperm is carefully inserted directly into the uterus through a thin catheter. This is done under the guidance of a pelvic ultrasound to ensure precise placement. The procedure is relatively quick and typically painless, though some women may experience mild cramping. The procedure can be performed at the usual doctor’s office.
After the procedure, the woman may be advised to rest for a few minutes before resuming normal activities. Blood tests are usually scheduled about 10-14 days later to check for pregnancy. A positive result is confirmed with a follow-up ultrasound.

The process begins with an initial consultation with a fertility specialist. The recipient undergoes a thorough evaluation to assess the health of her uterus, including blood tests to evaluate hormone levels and an ultrasound to examine the uterus and ovaries. A psychological assessment may also be recommended to ensure that the recipient is emotionally prepared for the use of donor eggs. Additionally, the donor undergoes her own medical screening, which typically includes genetic testing, infectious disease screening, and a fertility assessment to ensure that her eggs are of high quality.
Once the recipient’s medical evaluation is complete, the next step is selecting an egg donor. Donors are typically chosen from a donor bank, where their profiles, including medical history, genetic background, and physical traits, are available. Some recipients may choose to use an anonymous donor, while others may opt for a known donor (depending on the country’s law). The choice of donor is important, as it impacts both the genetic makeup of the embryos and the recipient’s emotional connection to the process.
The egg donor undergoes a process of ovarian stimulation, where she takes hormone injections (typically using gonadotropins) to encourage her ovaries to produce multiple eggs rather than the single egg that would be released in a natural cycle. The donor’s progress is closely monitored with blood tests and ultrasounds to track follicle growth. Once the follicles reach an optimal size (usually after 10-14 days of stimulation), a final injection of human chorionic gonadotropin (hCG) is given to trigger ovulation and the release of mature eggs.
Approximately 36 hours after the hCG injection, the donor undergoes an egg retrieval procedure, also known as oocyte aspiration. Under sedation, a needle is inserted through the vaginal wall and into the ovaries to collect the mature eggs. This is a minimally invasive procedure, and the donor is monitored during the recovery phase. Typically, multiple eggs are retrieved to increase the chances of successful fertilization.
Meanwhile, the recipient prepares for embryo implantation by undergoing hormone therapy, which typically includes estrogen and progesterone to stimulate the growth of the uterine lining (endometrium) and create an optimal environment for embryo implantation. This process may last several weeks, with regular monitoring to ensure the endometrium reaches the appropriate thickness for embryo transfer.
Once the eggs are retrieved from the donor, they are fertilized in the laboratory using sperm from the recipient’s partner (or a sperm donor, if necessary). The sperm and eggs are combined through conventional insemination or intracytoplasmic sperm injection (ICSI), where a single sperm is directly injected into each egg. The fertilized eggs (embryos) are cultured for several days, typically up to the blastocyst stage (5-6 days), to monitor their development and select the best quality embryos for transfer.
On the day of the embryo transfer, the best quality embryo is selected for implantation. A thin catheter is used to place the embryo into the recipient’s uterus, typically under ultrasound guidance to ensure precise placement. This procedure is usually painless, although some women may experience mild cramping afterward. If multiple embryos are available, the number transferred will depend on the age of the recipient and the quality of the embryos, as recommended by the fertility specialist.
After the embryo transfer, the recipient continues hormone therapy (e.g., progesterone) to support the uterine lining and facilitate implantation. About 10-14 days later, a blood test is conducted to check for pregnancy by measuring the levels of human chorionic gonadotropin (hCG), a hormone produced during pregnancy. If the test is positive, a follow-up ultrasound is typically scheduled after two weeks to confirm the pregnancy and check for a heartbeat. If the test is negative, the recipient may be advised to try another cycle.
If the pregnancy test is positive, the recipient will continue hormone treatment to maintain the pregnancy. The clinic will monitor the pregnancy with ultrasounds and blood tests to confirm its progression and detect any potential complications. Once the pregnancy is stable, care is typically transferred to an obstetrician for the remainder of the pregnancy.


The first step is a comprehensive evaluation of both partners’ fertility. This may involve blood tests to measure hormone levels, an ultrasound to assess the health of the ovaries and uterus, and a semen analysis to evaluate sperm quality. Based on these results, a treatment plan is developed.
To increase the number of eggs released during a woman’s cycle, ovulation is stimulated using fertility medications. The most common drugs used for this purpose are Clomiphene Citrate or injectable gonadotropins (e.g., FSH, LH). These medications encourage the ovaries to produce multiple follicles, each containing an egg, rather than just one egg as would occur in a natural cycle.
Throughout the stimulation phase, the woman undergoes regular monitoring through blood tests and ultrasounds. Blood tests track hormone levels (such as estradiol) to assess the ovaries’ response to the medications. Ultrasounds monitor the growth of the follicles to determine when they are ready for ovulation. Typically, the goal is to have 2-3 mature follicles for optimal chances of conception.
Once the follicles reach the appropriate size (usually around 18-20 mm), an injection of human chorionic gonadotropin (hCG) is administered to trigger ovulation. This hormone mimics the natural surge that would occur in a normal cycle, signaling the eggs to mature and be released from the follicles.
Intercourse are recommended on the same day of hCG injection and the day after. Timing intercourse at these moments maximizes the chances of sperm meeting the egg when it is released from the ovary.
About two weeks after ovulation, a blood test is performed to check for pregnancy. If the test is positive, a follow-up ultrasound is typically done around 6-7 weeks to confirm the pregnancy and assess its progress. If the result is negative, the couple can discuss next steps with their fertility specialist, which may include trying another cycle or considering alternative treatments.
Intrauterine insemination (IUI) with donor sperm is one of the simplest ART methods for achieving pregnancy. The process begins with the selection of a sperm donor. The donor sperm is obtained from a sperm bank, where it is rigorously screened for infectious diseases, genetic conditions, and quality. The sperm is then frozen and stored until it is needed for the IUI procedure.


The first step in the egg freezing process is an initial consultation with a fertility specialist. During this meeting, the doctor will discuss the woman’s reasons for egg freezing, medical history, and any potential fertility concerns. The doctor will also perform an assessment that includes blood tests to measure hormone levels (e.g., AMH – Anti-Müllerian Hormone, which gives an estimate of ovarian reserve), as well as an ultrasound to examine the ovaries and assess the quantity and quality of the remaining eggs. This evaluation helps the doctor understand the woman’s fertility status and determine the best approach for her egg freezing cycle.
To maximize the number of eggs retrieved, the woman undergoes ovarian stimulation using hormone injections. The most commonly used medications are gonadotropins, which stimulate the ovaries to produce multiple eggs rather than the single egg that would be released in a natural cycle. These hormones typically include follicle-stimulating hormone (FSH) and luteinizing hormone (LH). The stimulation process lasts about 10-14 days and is carefully monitored through regular blood tests and ultrasounds to track how the ovaries are responding. The goal is to develop multiple mature eggs for retrieval.
During the ovarian stimulation phase, the fertility clinic closely monitors the woman’s response to the medication. Ultrasound scans are used to check the growth of the ovarian follicles (fluid-filled sacs that contain the eggs), while blood tests measure hormone levels like estrogen and progesterone to ensure optimal follicle development. Based on the results, the medication dosage may be adjusted to maximize egg production while minimizing the risk of ovarian hyperstimulation syndrome (OHSS), a potential side effect of the stimulation.
When the follicles have reached the appropriate size (usually around 18-20 mm), an injection of GnRH agonist and/or human chorionic gonadotropin (hCG) is administered to trigger ovulation. This step prepares the eggs for retrieval. Ovulation is typically triggered 36 hours before the planned egg retrieval, which ensures that the eggs are mature and ready for collection.
Approximately 36 hours after the ovulation triggering, the woman undergoes the egg retrieval procedure, known as oocyte pick-up. This procedure is performed under light sedation or anesthesia and is minimally invasive. A thin needle is inserted through the vaginal wall and into the ovaries to harvest (remove) the mature eggs from the follicles. The procedure usually takes about 20-30 minutes. The woman may experience some cramping or discomfort after the procedure, but recovery is generally quick.
After the eggs are retrieved, they are carefully examined and prepared for freezing. The eggs are then cryopreserved through a process called vitrification, which involves rapidly freezing the eggs to prevent ice crystal formation and preserve their integrity. The eggs are stored in a cryogenic freezer at sub-zero temperatures until the woman is ready to use them in the future.
After the egg retrieval, the woman may be monitored for a short time to ensure there are no complications, such as ovarian hyperstimulation syndrome (OHSS). She may be advised to rest for the remainder of the day. In some cases, the woman may need a follow-up visit to ensure that her cycle has returned to normal.
When the woman is ready to use her frozen eggs—whether in her 30s, 40s, or later—the eggs are thawed and fertilized with sperm (either from a partner or a donor) through in vitro fertilization (IVF). The resulting embryos are cultured and then transferred into the woman’s uterus, with the goal of achieving pregnancy. The number of eggs retrieved and successfully frozen will impact the likelihood of a successful pregnancy later, so multiple rounds of egg retrieval may be recommended, especially if the woman is in her late 30s or older.
Frozen eggs can be stored for many years, depending on the fertility clinic’s regulations and the woman’s preferences. Many clinics allow egg storage for up to 10 years, and some offer options to extend storage beyond this period, with regular updates and consent renewal required from the woman.
As a woman ages, the quality of her eggs declines, which can lead to an increased risk of chromosomal abnormalities and miscarriage.

+972 58 63 68 585
jcohen.obgyn@gmail.com
Privacy Policy / © SCW-Studio / All Rights Reserved